Reply With Quote
Reply With Quote
You ers never gave a good about the Pope, 21, until now. Now, he's of use to you.

the one thing the daily show still does well is making these montage clips

You ers never gave a good about the Pope, 21, until now. Now, he's of use to you.
Not when they swear at President Trump and tell him it will be 3-5 years before FDA APPROVAL. "Maybe even longer." Then 7 months after Biden robs the Presidency FDA APPROVAL is delivered. No. that . Uh, uh.
i still dont give a about the pope. its all fake news anyway.
i just found the clip amusing

Good way for MAGA s to get three meals and a cot or maybe their humor does not translate well.
Woman who coughed on market produce, claimed virus gets jail.
WILKES-BARRE, Pa. (AP) — A Pennsylvania woman who pleaded guilty to coughing and spitting on food at a supermarket in the early days of the coronavirus pandemic was sentenced Tuesday to at least a year in jail.
Margaret Ann Cirko, 37, pleaded guilty in June to a felony count of making bomb threats.
Authorities said Cirko entered a Gerrity’s Supermarket location in Hanover Township, near Wilkes-Barre, on March 25, 2020, and purposely coughed on fresh produce and other merchandise while yelling that she had the virus and that everyone would get sick.
Joe Fasula, co-owner of the supermarket chain, said that over $35,000 worth of merchandise had to be thrown out as a result of what Gerrity’s had called a “twisted prank.
A Luzerne County judge called Cirko's conduct “totally outrageous" and sentenced her to one to two years in jail, to be followed by eight years of probation. She also was ordered to pay nearly $30,000 in res ution.
https://news.yahoo.com/woman-coughed...195309867.html

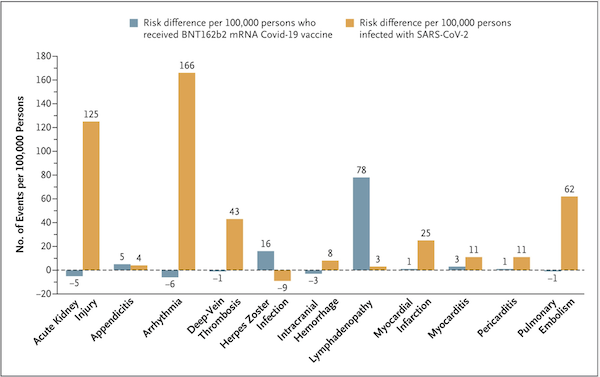
Israeli study of adverse outcomes of the Pfizer jab versus getting COVID, in the NEJM.
Looks like getting COVID is way more dangerous than vaccines except for shingles and swollen lymph nodes.
https://www.nejm.org/doi/full/10.1056/NEJMoa2110475
greed and vaccine diplomacy are prolonging the pandemic
https://www.ft.com/content/66adc278-...c-b33e915d4631
Winester, runnin' as fast as he can.
GO---Winester---GO!!!!!!!!!

Korispiracy
FLCCC guidelines, the one Karrin was pimping
Intellectual Derp Web strikes again
Right, you only care about what the alt right conspiracy nuts say

Great news if the rollout lines up with the trials; about 500,000 people die of malaria yearly
.
https://www.thetimes.co.uk/article/g...box=1629959087The jab, developed by the Brentford-based pharmaceutical company GSK, was found to reduce the rate of severe malaria by 70 per cent in a study involving nearly 6,000 children aged between five and 17 months in Burkina Faso and Mali.
Good discussion of respiratory infection via aerosols in Science Magazine, with an emphasis on engineering solutions.
http://science.sciencemag.org/content/373/6558/eabd9149Airborne transmission has long been an under-appreciated route for contributing to the transmission of respiratory viral diseases, largely because of an insufficient understanding of the generation and transport processes of virus-laden aerosols as well as misattribution of anecdotal observations. The epidemiological evidence for the dominance of airborne spread of SARS-CoV-2 has increased over time and has become especially strong. First, the distinct difference between indoor and outdoor transmission cannot be explained by droplet transmission because gravity-driven droplets behave identically indoors and outdoors. The high frequency of indoor superspreading events relative to those outdoors points to the importance of airborne transmission (63). The demonstrated role of poor ventilation in transmission and superspreading clusters indoors is also only compatible with aerosols, because droplets and fomite transmission are not affected by ventilation. Long-range airborne transmission of SARS-CoV-2 has been observed in hotel quarantines in countries with very low transmission (166) and in a large church (72).
During the emergence of novel respiratory viruses, a more holistic approach that acknowledges all modes of transmission (airborne, droplet, and fomite) is needed to successfully mitigate risk and prevent spread. The requirement for direct evidence of infectiousness of sampled aerosols before acknowledging and adding controls to address airborne transmission leaves people at potential risk (69). When unburdened by conventional definitions of transmission routes, the available evidence for SARS-CoV-2, influenza virus, and other respiratory viruses is much more consistent with transmission by aerosols <100 μm rather than by rare, large droplets sprayed onto mucous membranes of people in very close proximity. Recent acknowledgement of airborne transmission of SARS-CoV-2 by the WHO (48) and US CDC (49) reinforces the necessity to implement protection against this transmission route at both short and long ranges.
Once the mechanisms leading to airborne transmission are fully understood—acknowledging that transmission by aerosols is largest at close range—it becomes clear there is an overlap in precautions and mitigation measures for both droplets and aerosols (such as distancing and masks), but extra considerations must be taken into account for mitigating aerosol transmission at both short and long ranges. These include attention to ventilation, airflows, mask fit and type, air filtration, and UV disinfection, as well as distinguishing measures between indoor and outdoor environments. Although our knowledge is still increasing, enough is already known to add protective measures to better protect against airborne transmission of respiratory viruses, noting that “droplet precautions” are not replaced but instead expanded.
A high proportion of individuals infected with SARS-CoV-2 have no symptoms at the time of testing (167, 168). About 20 to 45% of individuals infected with SARS-CoV-2 remained asymptomatic throughout the course of infection, whereas some infected individuals experienced a presymptomatic phase and began to develop symptoms several days after infection (168, 169). The infectiousness of SARS-CoV-2 peaks two days before and extends to one day after symptom onset (170). High asymptomatic infection rates have also been reported for influenza virus and other respiratory virus infections (171–173). Although some studies suggest that airborne transmission is not an efficient route, particularly for asymptomatic and mildly symptomatic individuals who likely have low viral loads in their saliva (55), the viral load in presymptomatic individuals is comparable to that of symptomatic patients (174, 175). It is important to implement controls that protect against exposure of infectious virus-laden aerosols produced when infected individuals without any symptoms speak, sing, or simply breathe. Because these individuals do not know they are infected, they generally continue to be involved in social activities, leading to airborne transmission.
Universal masking is an effective and economical way to block virus-laden aerosols (67). Model simulations show that masks effectively prevent asymptomatic transmission and reduce the total number of infected individuals as well as mortalities as a result of COVID-19 (176). It is crucial to optimize the allocation of masks (177). Surgical masks have been shown to reduce the release of influenza virus, seasonal human coronaviruses, and rhinovirus in aerosols <5 μm into the air by infected individuals by up to 100% (104, 178), although for some individuals there was no reduction; and masks are more effective for limiting droplets (179). Masks made of combinations of different fabrics and/or multiple layers, when worn properly with no leaks, can block up to 90% of particles between 0.5 and 10 μm (179). Small gaps between the mask material and skin can lead to substantial decreases in the overall filtration efficiency. For aerosols <2.5 μm, filtration efficiency decreases by 50% for a relative leak area of 1% (180). A study compared the viral filtration efficiency of N95, surgical, and fabric masks using a model virus and found that the efficiency of N95 and some surgical masks exceeded 99%; all fabric masks tested were at least 50% efficient (181). The effectiveness of N95, surgical, and cotton masks in blocking SARS-CoV-2–containing aerosols has been investigated using manikins placed face-to-face. N95 respirators demonstrated the highest efficiency in blocking infectious SARS-CoV-2 (182). Almost all masks offer at least some protection, but they are not 100% effective. Transmission of SARS-CoV-2 has occurred in health care settings despite medical masks (designed for droplets not aerosols) and eye protection (183–185), which illustrates the need for proper personal protective equipment (PPE) and layering multiple interventions against airborne transmission, especially in high-risk indoor settings.
Health care facilities are more likely to accommodate patients infected with respiratory viruses. Thus, health care personnel should be provided with proper PPE to reduce airborne exposure. People occupying indoor spaces have increased potential to be exposed to high concentrations of virus-laden aerosols, especially in poorly ventilated and/or crowded indoor settings where virus-laden aerosols can readily ac ulate (93). Preventive measures should be implemented at all times when traveling in airplanes, trains, buses, ships, and cruise ships, which have relatively small and enclosed air spaces where the ventilation may not always be optimal. Many studies indicate that the risk of airborne transmission in outdoor environments is substantially lower than indoor environments (186); however, the risk of transmission outdoors exists in close proximity situations, especially if talking, singing, or shouting over time. The risk of outdoor transmission may rise with increased lifetime and transmissibility of viruses, such as certain variants of SARS-CoV-2 (187, 188). Aerosolization of virus-containing wastewater and hospital fecal discharges also poses potential outdoor exposure risks, which should not be underestimated (189).
Implementing effective ventilation systems reduces airborne transmission of infectious virus-laden aerosols. Strategies such as ensuring sufficient ventilation rates and avoiding recirculation are advised (190, 191). Carbon dioxide sensors can be used as indicators of the build-up of exhaled air and serve as a simple way to monitor and optimize ventilation (192, 193). Aerosol sensors can also be used to assess HEPA and HVAC aerosol filtration efficiencies, which are key to lowering infections caused by virus-laden aerosols. Assuring a minimum ventilation rate of 4 to 6 air changes per hour (ACH) and maintaining carbon dioxide levels below 700 to 800 ppm have been advised, although the ventilation type and airflow direction and pattern should also be taken into account (148, 194). Increasing the efficiency of air filtration in HVAC systems, stand-alone HEPA purifiers, or implementing upper room UV disinfection systems can further reduce the concentrations of virus-laden aerosols (47, 127, 140, 141, 195).
Physical distancing, a mitigation put in place to address droplet transmission, is also effective in reducing the chances of aerosol inhalation because aerosol concentrations are much higher in close proximity to an infected individual (50). The WHO and many national public health agencies recommend maintaining physical distances of either 1 or 2 m. However, this distance is not sufficient to protect against aerosols that travel beyond this range. If large droplets dominated transmission, distancing alone would have effectively suppressed the transmission of SARS-CoV-2. As has been repeatedly shown in superspreading events, airborne transmission occurs in poorly ventilated rooms when occupants inhale infectious room air (18, 36, 62, 64, 71). Additionally, although distancing helps by moving people away from the most concentrated parts of respiratory plumes, distancing alone does not stop transmission and is not sufficient without accounting for other measures, such as ventilation and filtration, the number of people emitting infectious aerosols, and the amount of time spent in enclosed spaces (196). The unknown number of asymptomatic (including presymptomatic) infected individuals present in specific environmental settings is an additional challenge in respiratory disease control. Engineering measures to reduce aerosol concentrations through ventilation, filtration, and upper room UV disinfection remain critical strategies for reducing airborne transmission risks.
Despite the emerging recognition of airborne transmission of respiratory viruses, numerous issues require further exploration. For example, direct measurements are needed of the concentration of virus in aerosols and droplets as a function of size and their potential to initiate a new infection. The lifetime of viruses in aerosols of varying size requires systematic investigation. More studies are needed to quantify the relationship between viral dose delivered by aerosols and droplets and severity of infection; this relationship likely varies considerably for different viruses. It is also important to investigate whether the severity of disease correlates with the size and number of aerosols and the location in which they are deposited in the respiratory tract. Although more studies are needed, unequivocal evidence indicates that airborne transmission is a major pathway for the spread of SARS-CoV-2 and many other respiratory viruses. Additional precautionary measures must be implemented for mitigating aerosol transmission at both short and long ranges, with a major focus on ventilation, airflows, air filtration, UV disinfection, and mask fit. These interventions are critical strategies for helping end the current pandemic and preventing future outbreaks. It is important to note that these proposed measures to improve indoor air quality will lead to long overdue improvements that have health benefits extending well beyond the COVID-19 pandemic.
thread
yea, TSA posted this "bombs " a couple of days ago.

What's your point?

read the responses between the readers and the OP in the second snapshot
Maybe I'm missing something. That paper studied 3 groups.
Here's how I interpreted their conclusion
Infected + single shot >> Infected >> Double vaxxed
very good!
you caught what the OP, Mr Blumental, did not

There are currently 2 users browsing this thread. (0 members and 2 guests)
 Posting Permissions
Posting Permissions