Reply With Quote
Reply With Quote
^Yesterday will take care that.

first tick down we've seen in a bit on the national graphs


^Yesterday will take care that.

Yeah, might just be a holiday pause like Thanksgiving. Austin hospitalizations had just gone into Stage 5 territory Wednesday and won't report again until Monday.
I'd put my money on that. You can see reported deaths/cases drop after every holiday, and I'm sure this is the case again.
Yeah I'm worried because the number of new hospitalizations was really starting to take off. It's so strange that they can't/won't compile the numbers every day.

And it'll be a huge jump in about a week. And then another jump a week later from New Year's. January promises to be a monumental cluster .
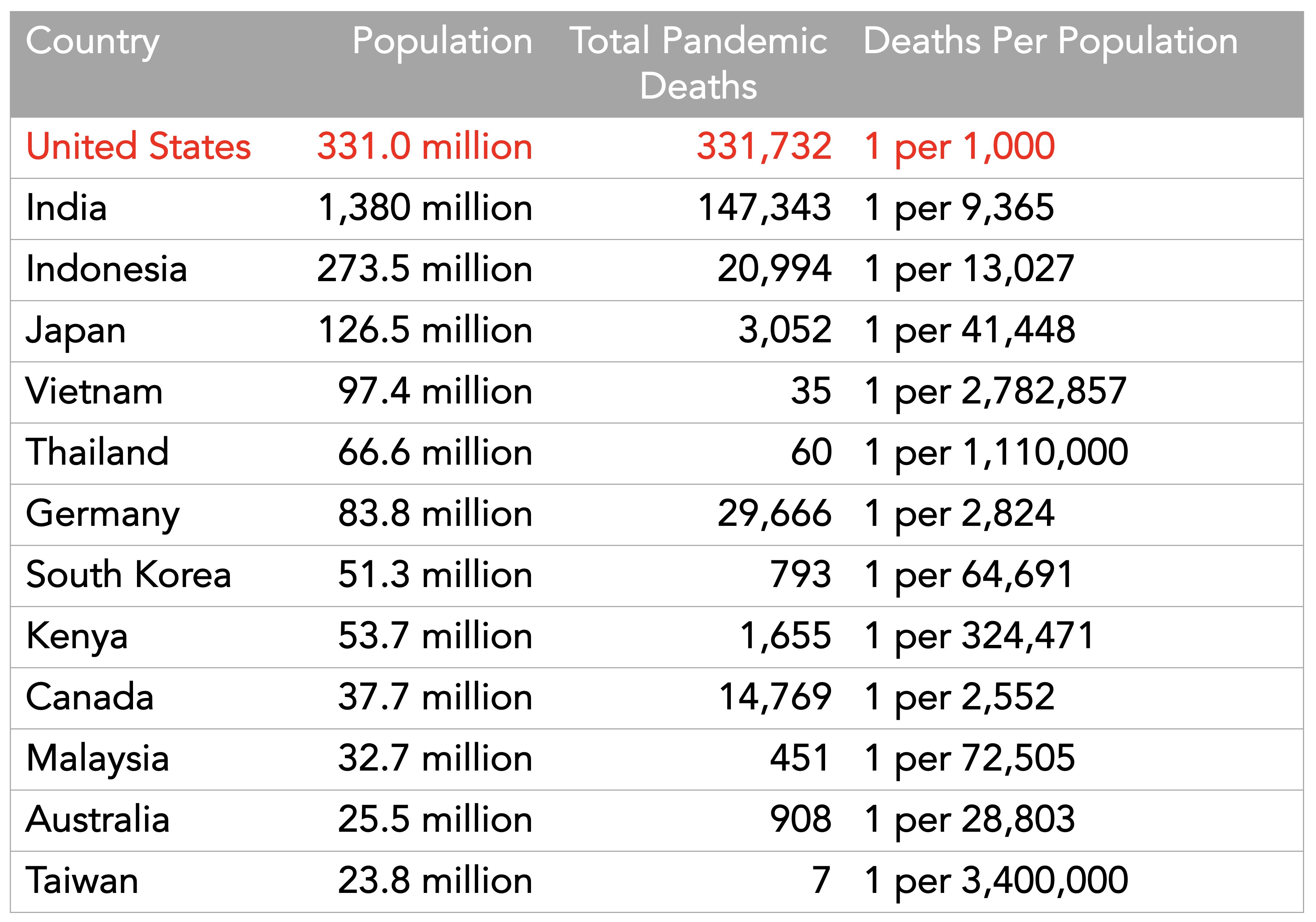
only four countries with more than 20 million people have had it worse than the USA

think of all the people not listed as 9/11 casualties. way more than 99% of Americans.
why are you still whining about it?
Rationing care in SoCal has begun. Still some NICU, teen psych beds, and space in the In-N-Out parking lot available so all good.
I can't think of a swear strong enough. This is horrible.

This is the foldren's backup for ICUs available in all hospitals.
Hospital could be his neighborhood and ICUs found in his various closets.
badong... killing is badong
Austin's number has it back where it was in early July. It's insane that they take weekends and holidays off when we've just gone into the highest stage of alert. Three days of no reporting at all is complete bull and it's going to happen again this week.
Some Austin numbers before the 6PM stat dump. Not great:
As of Monday, there are 4,411 active cases in the area, including 404 hospitalizations. It’s just shy of a week since Austin-Travis County moved to Stage 5 of COVID-19 risk-based guidelines due to uncontrolled spread.
Escott said the average of new hospital admissions is up 106% since the beginning of December, and new admissions to intensive care units are up 62% since a week ago. Escott said at this rate, ICUs in the area could run out of beds in a week.
“We’ve seen dramatic utilization in ICUs in the past week, and that’s where we have the most limited resources,” Escott said. “There’s plenty of equipment available. The issue is the staffing.”
https://www.kxan.com/news/local/aust...vid-19-update/
why is Austin so much lower than even SA?
My guess is more working from home and better guideline discipline, but it's all breaking down so we're probably just behind SA rather than lower.

... and there it is.
Whoopski!
sex and metabolic comorbidities
n=66,646
https://academic.oup.com/cid/advance...aa1787/6041643Among 66,646 (6.5%) admissions with a COVID-19 diagnosis, across 613 U.S. hospitals, 12,388 (18.6%) died in-hospital. In multivariable analysis, male sex was independently associated with 30% higher mortality risk (aRR, 1.30, 95% CI: 1.26 – 1.34). Diabetes without chronic complications was not a risk factor at any age (aRR 1.01, 95% CI: 0.96 – 1.06), and hypertension without chronic complications was only a risk factor in 20-39 year-olds (aRR, 1.68, 95% CI: 1.17 – 2.40). Diabetes with chronic complications, hypertension with chronic complications, and obesity were risk factors in most age-groups, with highest relative risks among 20-39 year-olds (respective aRRs 1.79, 2.33, 1.92; p-values ≤ 0.002).
Conclusions
Hospitalized men with COVID-19 are at increased risk of death across all ages. Hypertension, diabetes with chronic complications, and obesity demonstrated age-dependent effects, with the highest relative risks among adults aged 20-39.
sex and metabolic comorbidities
n=66,646
https://academic.oup.com/cid/advance...aa1787/6041643Among 66,646 (6.5%) admissions with a COVID-19 diagnosis, across 613 U.S. hospitals, 12,388 (18.6%) died in-hospital. In multivariable analysis, male sex was independently associated with 30% higher mortality risk (aRR, 1.30, 95% CI: 1.26 1.34). Diabetes without chronic complications was not a risk factor at any age (aRR 1.01, 95% CI: 0.96 1.06), and hypertension without chronic complications was only a risk factor in 20-39 year-olds (aRR, 1.68, 95% CI: 1.17 2.40). Diabetes with chronic complications, hypertension with chronic complications, and obesity were risk factors in most age-groups, with highest relative risks among 20-39 year-olds (respective aRRs 1.79, 2.33, 1.92; p-values ≤ 0.002).
Conclusions
Hospitalized men with COVID-19 are at increased risk of death across all ages. Hypertension, diabetes with chronic complications, and obesity demonstrated age-dependent effects, with the highest relative risks among adults aged 20-39.
Disparity of impact: hospitalization rates and relative mortality are markedly worse and trend much younger among African Americans and non-white Hispanics
Findings from other published studies are consistent with COVID-NET data. Across several studies, most found a higher percent of hospitalized patients were non-Hispanic Black or Hispanic or Latino people than non-Hispanic White people.
Race or Ethnicity Group Percent of hospitalized COVID-19 patients Median [Range] # of Studies Reporting Black 44% [1581%] 7 1,2,3,4,5,6,7 Hispanic or Latino 36% [348%] 4 1,2,3,4 White 16% [1172%] 6 1,2,4,5,6,7
Notes: Studies reporting data on percent of hospitalized patients by race and ethnicity included people of all ages. These studies analyzed race and ethnicity differently; two studies analyzed the variables separately (racial categories could be Hispanic or Latino or non-Hispanic) and five studies analyzed the variables in a single variable (racial categories were non-Hispanic). Data were inadequate to assess potential differences in percent of hospitalized COVID-19 patients for American Indian and Alaska Native people, Native Hawaiian and other Pacific Islander people, and people who identify with more than one race. Therefore, data for these groups are not reported.
Acute kidney injury has been a common outcome among patients hospitalized with COVID-19. One study found that among patients hospitalized with COVID-19, 37% developed acute kidney injury. Among those with acute kidney injury, 35% died compared with 16% of all patients hospitalized with COVID-19. Acute kidney injury was more likely among Black patients than White patients. 8
Severe illness from COVID-19 is disproportionately affecting children and adolescents from racial and ethnic minority groups. Multisystem inflammatory syndrome in children (MIS-C) is a rare but severe condition that occurs approximately 24 weeks after the onset of COVID-19 in children and adolescents. MIS-C disproportionately affects children and adolescents from racial and ethnic minority groups. 9, 10 More than 70% of reported cases have occurred among children who are Hispanic or Latino or non-Hispanic Black. Data are routinely monitored and updated here.
To prevent severe illness from COVID-19, we need to work together to address inequities in the social determinants of health that increase risk of severe illness from COVID-19 for racial and ethnic minority groups. Learn more about what we can do to move towards health equity.
https://www.cdc.gov/nchs/nvss/vsrr/covid19/health_disparities.htm
https://www.cdc.gov/coronavirus/2019...ies/index.html
https://www.dallasnews.com/news/2020...f-their-lives/
hospitalizations still going up

41 year old Congressman-elect dies of COVID-19
https://www.nytimes.com/2020/12/29/w...lications.html
There are currently 1 users browsing this thread. (0 members and 1 guests)
 Posting Permissions
Posting Permissions